

What is Juvenile-Onset Idiopathic Arthritis?
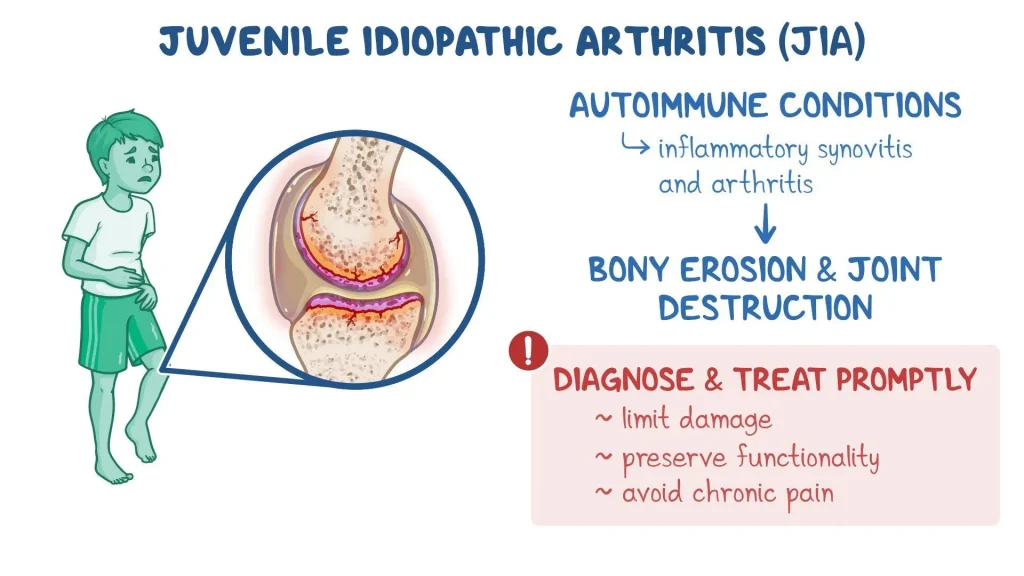
Juvenile-Onset Idiopathic Arthritis (JIA) is a chronic autoimmune condition that affects children under the age of 16. It causes inflammation in one or more joints, leading to pain, stiffness, swelling, and reduced mobility. The term “idiopathic” means the exact cause is unknown.
JIA is the most common type of arthritis in children and can range from mild to severe, with some cases resolving over time and others lasting into adulthood.
What causes it?
The exact cause of JIA is unknown, but it is believed to involve a combination of genetic and environmental factors. The immune system mistakenly attacks the body’s own joint tissues, leading to inflammation.
It is not contagious, and it is not caused by injuries or infections, although certain infections may trigger symptoms in genetically predisposed children.
What are the types?
JIA includes several subtypes:
- Oligoarticular JIA: Affects 4 or fewer joints; most common type
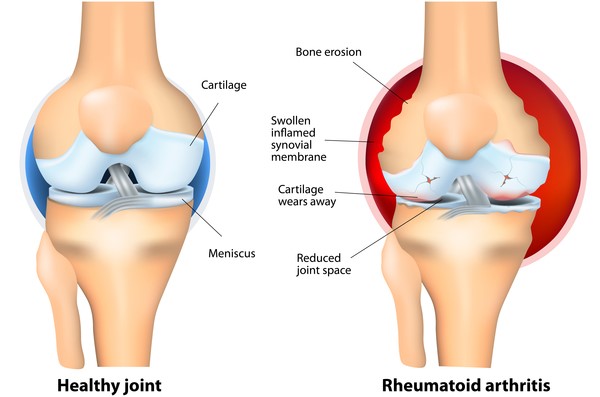
- Polyarticular JIA: Affects 5 or more joints; may resemble adult rheumatoid arthritis
- Systemic JIA (Still’s disease): Affects the whole body, with fevers, rash, and internal organ involvement
- Enthesitis-related JIA: Involves the tendons and ligaments as well as joints
- Psoriatic JIA: Occurs in children with psoriasis or a family history of it
What are the symptoms?
Symptoms can vary depending on the subtype but often include:
- Joint pain, especially in the morning
- Swelling and warmth in the joints
- Stiffness that may improve with activity
- Fatigue and reduced physical activity
- Limping or difficulty using a limb
- Fevers, rash, or eye inflammation (in systemic cases)
How is it diagnosed?
There is no single test for JIA, so diagnosis involves:
- Physical examination to assess joint function and inflammation
- Blood tests to check for inflammation and rule out other conditions (e.g., ANA, ESR, CRP, rheumatoid factor)
- Imaging tests like X-rays, ultrasound, or MRI to evaluate joint damage
- Eye exams, especially if the child is at risk for uveitis (eye inflammation)
How is it treated?
Treatment focuses on reducing inflammation, managing symptoms, and maintaining joint function:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce pain and inflammation
- Disease-modifying antirheumatic drugs (DMARDs) like methotrexate
- Biologic agents that target specific immune responses (e.g., TNF inhibitors)
- Steroids, used cautiously for severe flare-ups
- Physical and occupational therapy to maintain joint mobility and muscle strength
Early and aggressive treatment can significantly improve outcomes.
What is the prognosis?
Many children with JIA go into remission with proper treatment, especially if the condition is diagnosed early. Some children may have long-term symptoms or joint damage, particularly in more severe cases.
Regular follow-up and a personalized treatment plan are essential for managing the condition and improving quality of life.
When should I see a doctor?
You should consult a pediatrician or rheumatologist if your child experiences:
- Persistent joint pain or swelling
- Morning stiffness lasting more than 30 minutes
- Unexplained fever or fatigue
- A noticeable limp or decreased activity
- Eye redness or discomfort
Early diagnosis and intervention are key to preventing complications and supporting healthy growth.