

What is Acute Necrotizing Encephalopathy (ANE)?
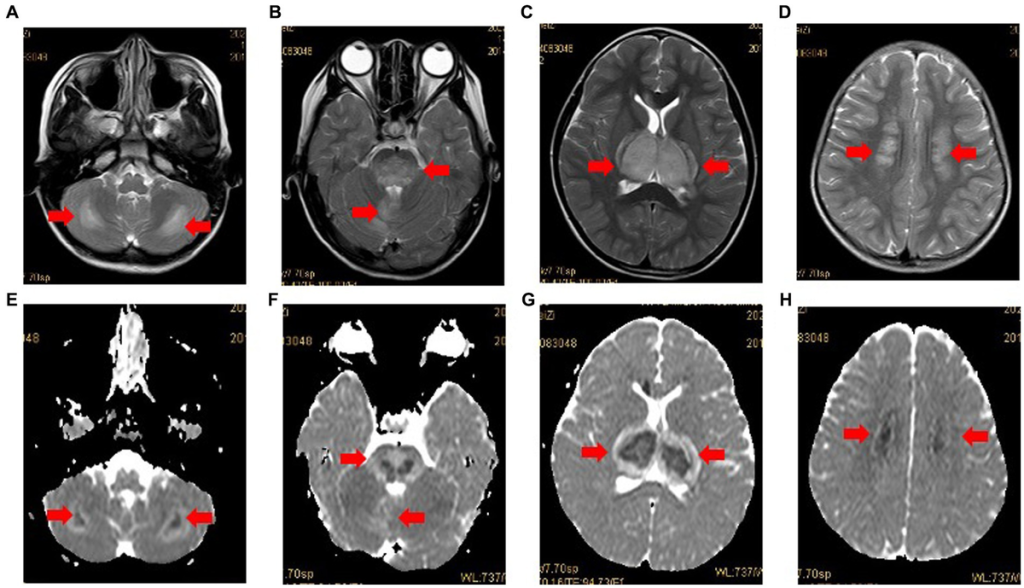
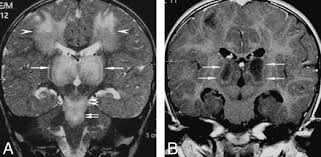
Acute Necrotizing Encephalopathy (ANE) is a rare and severe neurological disorder that primarily affects the brain. It is characterized by rapidly progressing brain inflammation, leading to symmetrical brain lesions in areas such as the thalamus, brainstem, and cerebellum.
ANE is most commonly seen in children but can also affect adults. It is typically triggered by viral infections, such as influenza or other respiratory illnesses. The condition progresses rapidly and can lead to coma, neurological disability, or even death if not treated promptly.
What Causes Acute Necrotizing Encephalopathy?
The exact cause of ANE is not fully understood, but it is believed to be an immune-mediated response to viral infections. Common triggers include:
- Influenza (Flu virus) – Most common trigger
- Human herpesvirus 6 (HHV-6)
- Enterovirus
- Respiratory syncytial virus (RSV)
- SARS-CoV-2 (COVID-19) and other coronaviruses
Instead of directly attacking the brain, these viruses cause an overactive immune response leading to widespread inflammation and brain damage.
Genetic Links (ANE1)
Some cases of ANE are linked to genetic mutations in the RANBP2 gene, known as ANE1, which increases susceptibility to severe neurological inflammation after infections.
Who is at Risk for ANE?
Anyone can develop ANE, but certain factors increase the risk:
- Children under 5 years old – Most common age group affected.
- Genetic predisposition – Mutations in the RANBP2 gene increase risk.
- Recent viral infections – Especially flu and other respiratory viruses.
- Weakened immune system – Conditions affecting immune response may contribute.
What Are the Symptoms of Acute Necrotizing Encephalopathy?
ANE symptoms progress rapidly, often within 24 to 48 hours after a viral infection. Early symptoms resemble a typical viral illness but quickly worsen into neurological complications.
Early Symptoms (Before Neurological Involvement)
- Fever
- Cough, sore throat, or other flu-like symptoms
- Vomiting and diarrhea
- Fatigue and weakness
Neurological Symptoms (Rapid Onset)
- Altered mental status (confusion, disorientation)
- Seizures
- Loss of consciousness or coma
- Difficulty moving or speaking
- Abnormal muscle stiffness or weakness
- Lack of coordination (ataxia)
Without immediate treatment, permanent brain damage, coma, or death may occur.
How is Acute Necrotizing Encephalopathy Diagnosed?
ANE is diagnosed through clinical evaluation, imaging tests, and laboratory studies:
- Magnetic Resonance Imaging (MRI) – The key diagnostic tool. It shows bilateral symmetric lesions in the thalamus, brainstem, and other brain regions.
- Lumbar Puncture (Spinal Tap) – May show elevated protein but normal white blood cell count in cerebrospinal fluid (CSF).
- Blood Tests – To check for viral infections, inflammatory markers, and metabolic abnormalities.
- Genetic Testing – If ANE1 is suspected, testing for RANBP2 gene mutations may be performed.
What Are the Treatment Options for Acute Necrotizing Encephalopathy?
There is no specific cure for ANE, but early and aggressive treatment can improve outcomes.
Main Treatment Approaches
- High-dose corticosteroids (e.g., methylprednisolone) – Reduce brain inflammation.
- Intravenous immunoglobulin (IVIG) – Helps modulate the immune response.
- Plasmapheresis (Plasma exchange therapy) – Removes harmful immune components.
- Antiviral medications – If a specific virus is identified.
- Supportive care – Includes mechanical ventilation, seizure control, and intensive care monitoring.
Long-Term Management
- Neurological rehabilitation – Physical therapy, speech therapy, and cognitive therapy for patients with lingering deficits.
- Genetic counseling – Recommended for families with ANE1 mutations.
What is the Prognosis for Acute Necrotizing Encephalopathy?
The prognosis of ANE varies depending on:
- How early treatment is started
- The severity of brain lesions seen on MRI
- Presence of genetic mutations (ANE1 cases tend to have recurrent episodes)
Possible Outcomes
- Mild cases: Some patients recover with minimal or no lasting damage.
- Moderate cases: Long-term neurological deficits such as cognitive impairment or movement disorders.
- Severe cases: Coma, severe disability, or death in cases with extensive brain damage.
Mortality rate: ANE has a high fatality rate (30-50%) in severe cases, but early intervention improves survival chances.
Can Acute Necrotizing Encephalopathy Be Prevented?
While ANE itself cannot always be prevented, the following measures may reduce the risk:
Viral Infection Prevention
- Annual flu vaccination – Reduces the risk of flu-triggered ANE.
- Good hygiene – Frequent handwashing, avoiding sick individuals.
- COVID-19 precautions – Masking and vaccination for high-risk individuals.
Genetic Screening for ANE1
- Families with a history of recurrent ANE cases should consider genetic counseling.
- Individuals with RANBP2 mutations should take extra precautions during viral infections.