

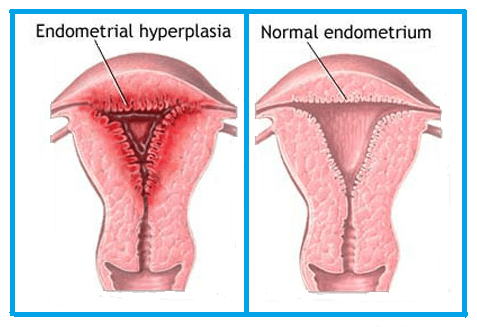
What is Endometrial Hyperplasia?
Endometrial hyperplasia is a condition where the lining of the uterus (the endometrium) becomes thickened due to an overgrowth of cells. This condition often occurs when there is an imbalance between the hormones estrogen and progesterone. Estrogen stimulates the endometrium to grow, and progesterone helps to regulate that growth. When there is too much estrogen and not enough progesterone, the lining of the uterus can become abnormally thick, which may lead to abnormal bleeding and other complications.
Endometrial hyperplasia can be classified into different types based on the degree of cellular abnormality. In some cases, the condition can lead to the development of endometrial cancer, although not all forms of endometrial hyperplasia progress to cancer.
What Are the Causes and Risk Factors of Endometrial Hyperplasia?
Endometrial hyperplasia is primarily caused by an imbalance in the hormonal cycle, particularly an excess of estrogen without the balancing effect of progesterone. The following factors can increase the risk of developing endometrial hyperplasia:
1. Hormonal Imbalances:
- An excess of estrogen or a deficiency of progesterone is the most common cause of endometrial hyperplasia.
2. Polycystic Ovary Syndrome (PCOS):
- Women with PCOS often have irregular menstrual cycles and higher levels of estrogen, which can increase the risk of endometrial hyperplasia.
3. Obesity:
- Obesity can lead to increased levels of estrogen in the body, as fat tissue can convert other hormones into estrogen, which may contribute to the development of endometrial hyperplasia.
4. Menopause:
- Perimenopause and postmenopause are times when hormonal imbalances are more likely to occur. Low levels of progesterone and fluctuating estrogen levels can increase the risk of endometrial thickening.
5. Estrogen Replacement Therapy (ERT):
- Women who are undergoing hormone replacement therapy (HRT) for menopause symptoms, especially if they are taking estrogen without progesterone, are at higher risk.
6. Infertility Treatments:
- Some fertility treatments that involve estrogen stimulation, such as in vitro fertilization (IVF), may increase the risk of endometrial hyperplasia.
7. Family History:
- A family history of endometrial cancer, ovarian cancer, or colon cancer may increase the risk of endometrial hyperplasia.
8. Age:
- Endometrial hyperplasia is more common in women over the age of 35, particularly those who have entered perimenopause or menopause.
9. Diabetes:
- Women with diabetes are at a higher risk of hormonal imbalances, which may contribute to the development of endometrial hyperplasia.
What Are the Symptoms of Endometrial Hyperplasia?
The symptoms of endometrial hyperplasia can vary depending on the severity of the condition. Common symptoms include:
1. Abnormal Uterine Bleeding:
- Heavy periods, irregular bleeding, or bleeding between periods are the most common symptoms. Some women may experience prolonged bleeding or spotting.
2. Postmenopausal Bleeding:
- Any bleeding that occurs after menopause is a red flag for potential endometrial issues, including endometrial hyperplasia.
3. Pelvic Pain:
- Although not always present, some women may experience discomfort or pelvic pain due to the thickening of the uterine lining.
4. Menstrual Irregularities:
- Changes in the frequency, duration, or intensity of menstrual cycles, including missed periods, can be a symptom of endometrial hyperplasia.
5. Infertility:
- Women with endometrial hyperplasia may have difficulty conceiving due to changes in the uterine lining that interfere with embryo implantation.
How is Endometrial Hyperplasia Diagnosed?
Diagnosis of endometrial hyperplasia typically involves a combination of physical examination, imaging tests, and procedures to examine the uterine lining:
1. Pelvic Examination:
- During a pelvic exam, a healthcare provider may check for signs of abnormal uterine growth or other conditions that could be causing abnormal bleeding.
2. Ultrasound:
- A transvaginal ultrasound can be used to measure the thickness of the endometrium. A thickened endometrial lining may suggest hyperplasia or other conditions.
3. Endometrial Biopsy:
- An endometrial biopsy involves removing a small sample of tissue from the uterine lining to examine under a microscope. This is the most definitive test for diagnosing endometrial hyperplasia.
4. D&C (Dilation and Curettage):
- In some cases, a D&C may be performed to remove a sample of the endometrial tissue for further examination, particularly if the biopsy results are unclear.
5. Hysteroscopy:
- A hysteroscope (a thin tube with a camera) can be inserted into the uterus to directly visualize the endometrial lining and to remove tissue samples if needed.
6. Hormonal Assessment:
- Blood tests may be conducted to check hormone levels, including estrogen and progesterone, to identify any imbalances contributing to endometrial hyperplasia.
How is Endometrial Hyperplasia Treated?
Treatment for endometrial hyperplasia depends on the type of hyperplasia, the severity, and whether or not the condition is precancerous. The main treatment options include:
1. Progestin Therapy:
- Progestin (a synthetic form of progesterone) is commonly used to counteract the effects of excess estrogen and help normalize the endometrial lining. This treatment may be prescribed in pill, injection, or intrauterine device (IUD) form.
2. Hormonal Therapy:
- Hormonal treatments such as birth control pills or a combination of estrogen and progesterone may be used to regulate menstrual cycles and reduce the risk of hyperplasia.
3. Surgical Options:
- Hysterectomy (removal of the uterus) is often recommended for women with severe or complex endometrial hyperplasia, especially if the condition is precancerous or involves a high risk of developing into endometrial cancer.
4. Endometrial Ablation:
- For women who are not planning to have children, endometrial ablation may be recommended. This procedure involves destroying the lining of the uterus to reduce bleeding.
5. Lifestyle Changes:
- Weight loss and management of underlying conditions like diabetes or PCOS can help regulate hormones and reduce the risk of endometrial hyperplasia.
6. Close Monitoring:
- In some cases, particularly for mild forms of hyperplasia, close monitoring with regular follow-up visits may be recommended to track the condition and prevent progression.
When Should You See a Doctor About Endometrial Hyperplasia?
You should see a doctor if you experience any of the following symptoms:
- Heavy or irregular menstrual bleeding.
- Postmenopausal bleeding or spotting.
- Pelvic pain or discomfort.
- Difficulty conceiving.
It’s important to seek medical attention if you notice any changes in your menstrual cycle, as early diagnosis and treatment of endometrial hyperplasia can help prevent complications, including endometrial cancer.